
Walking the journey with our patients
6 MINUTE READ
From Luke’s Journal 2021 | Children of God | Vol.26 No.3

Miscarriage and early pregnancy loss is often an emotionally taxing and devastating season in a woman’s life.
Early pregnancy loss is described as loss of a pregnancy under 20 weeks of gestation, and can include miscarriage, ectopic pregnancy and molar pregnancies.1 It affects 10-20% of clinical pregnancies, and is often a distressing situation for couples, where the initial excitement and joy can turn quickly into shock, disbelief and sadness.
There are well-defined ultrasound criteria to diagnose miscarriage, namely an embryo measuring 7mm or greater without the presence of a heart beat, a gestational sac diameter of 25mm or greater without an embryo, or lack of progress on successive ultrasound scans.2,3
Recurrent miscarriage is defined as three consecutive pregnancy losses, and can have a range of causes including structural uterine anomalies (e.g. fibroids, septum, adhesions), anti-phospholipid syndrome, diabetes, thyroid disease, genetic or chromosomal factors.
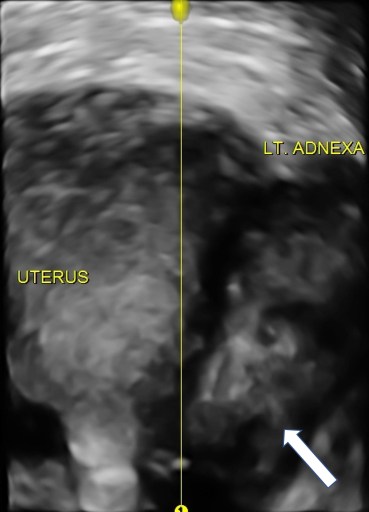
It is important to also recognise that though not classified as miscarriage, molar and ectopic pregnancies also are an experience of early pregnancy loss for a woman, and where there is a visible embryo or fetal heart activity, this can be a very distressing situation where the woman faces moral dilemma with her treatment options.
Treatment options for early pregnancy loss
Tailoring management is often a balance between what is clinically safe and what a woman feels is acceptable – empowering the patient with the knowledge to make an informed choice helps to engage her in an active decision-making process.
Miscarriages are commonly managed through primary care settings or within an early pregnancy hospital service. It can be managed expectantly if at an early gestation, the woman has access to transport to the hospital, and lives locally. Though this is the least invasive option, it often takes the longest period of time and can be associated with a need for repeat ultrasound scans and further treatment. Some women wish for as little intervention as possible, and prefer to wait it out. For others, they cannot bear the thought of waiting without a known endpoint.
Medical management suits women who are willing to hasten the miscarriage process, and usually offers a quicker outcome than expectant management. The combination of mifepristone and misoprostol, available to licensed prescribers, causes uterine contractions and can be associated with intense cramping and heavy bleeding.
Surgical management involves a general anaesthetic and uterine curettage, and may be the only safe available option for someone who has a more advanced pregnancy, lives further away, and with all molar pregnancies due to the high risk of hemorrhage. Repeated curettage can increase the risk of Asherman’s syndrome (uterine adhesions) and future infertility.

Ectopic pregnancies can be managed medically with methotrexate, or surgically, depending on the location of the pregnancy, bHCG and clinical presentation. It can lead to a life threatening situation if unmanaged, with rupture of the pregnancy and hemorrhage.
Whichever the treatment route, Anti-D is recommended for all women who are Rhesus negative, along with the offer for supportive and counselling services.
What role do I have?
Primum non nocere – First do no harm4
At whichever point of care, be it in primary, secondary or tertiary, it is important firstly to establish the correct diagnosis. Sometimes this is a straightforward process, either through an ultrasound meeting set criteria, or consecutively declining hormone (bHCG) levels. Where there is any doubt and the diagnosis is not definitive, a repeat ultrasound or bHCG does no harm, and a second opinion can be helpful. Just as there is a wide variation in life of what is considered “normal”, so too is there in early pregnancy – “late bloomers” do exist!
Once certain of the diagnosis, offer an empathetic approach, because to the woman it is the loss of a dream, the loss of a life and the loss of unrealised potential. Every woman grieves differently – some readily accept that this is a fact of life and unfortunate circumstances happen to all. Others, especially those who have been long awaiting this pregnancy, through IVF or other assisted reproductive efforts, struggle deeply to accept the situation before them, and experience emotions ranging from disbelief, guilt, anger, and sadness.
“Medical training helps us to understand and treat many things, but there is much we still cannot explain.”
Medical training helps us to understand and treat many things, but there is much we still cannot explain. Women commonly ask, “Why did this happen?”, “Will this happen again?” and sometimes the honest answer is that we do not know.
Not having every answer is a humbling part of our profession, but it helps us look beyond ourselves and acknowledge the fact that we are but His hands and feet in this world, and we are not called to know all the answers, but to diligently walk in obedience where God has placed us.
Sometimes the fear of not having all the answers causes us to withdraw and quieten our communication, but in doing so we amplify the echoing silence that the woman already feels. As believers, we can stand on God’s truth for our patients, offer to pray with them, and (regardless of their faith) offer hope and support through their journey of grief and loss. We can trust in God’s goodness and perfect will in their lives, and that His plan is to “maketh the barren woman to keep house, and to be a joyful mother of children.” (Ps 113:9 KJV).
The next pregnancy
Many women are keen to try for another pregnancy as soon as they are able. Others need time to grieve and adjust before trying again. This is often an opportune time to optimise medical comorbidities, encourage the cessation of smoking, alcohol and recreational drugs, and ensure they are up to date with their health screening. Women who have had recurrent miscarriage would benefit from a karyotype, thrombophilia & antiphospholipid screen, and a 3D pelvic ultrasound.

Though women with early pregnancy loss have a skewed perspective on what is normal, I do often remind them that “common things are common” and that despite their experience, it is still more likely that their next pregnancy will be one that implants and progresses normally. It is recommended that an early serum bHCG is performed as soon as the patient has a positive home pregnancy test, and a formal ultrasound arranged for reassurance.
What is more important than being able to solve their medical problems is our willingness and ability to walk that journey with our patients and support them through it. What a privilege! Helping them to process that grief, overcome fear of the known and unknown, and find the courage to move forward with hope is a calling both in the medical profession and as a believer. It is as much a journey for us, as it is for them.
“For God has not given us a spirit of fear, but of power and of love and of a sound mind.”(2 Tim 1:7)

Dr Gracia Chong Dr Gracia Chong is a gynaecologist in Newcastle. Her diploma in diagnostic ultrasound drives her keen involvement in tertiary gynaecology and early pregnancy scanning. She is a mother of two, avid urban gardener, and enjoys playing keys for her church’s creative music team.
References:
- Sands Australia, http://www.sands.org.au, accessed 8 August, 2021.
- Preisler J, Kopeika J, Ismail L, Vathanan V, Farren J, Abdallah Y, et al. Defining safe criteria to diagnose miscarriage: prospective observational multicentre study. BMJ. 2015;351:h4579.
- Australasian Society for Ultrasound in Medicine. Guidelines for the performance of first trimester ultrasound. Sydney: ASUM, 2014.
- Hughes G. First do no harm; then try to prevent it. Emerg Med J. 2007;24(5):314.
Would you like to contribute content to Luke’s Journal? Find out more…


